Introduction
The world faces an unprecedented urban health crisis. By 2050, approximately 68% of humanity will live in cities, with 90% of this growth concentrated in Africa and Asia (United Nations Department of Economic and Social Affairs, 2018). This explosive urbanization creates a basic challenge: while cities historically drove improvements in public health through economies of scale and infrastructure investment, today’s fastest-growing cities lack the capital, time, and institutional capacity to replicate traditional development pathways.
Traditional healthcare infrastructure development follows a well-established pattern: build road networks connecting facilities, ensure reliable electrical grids, construct hospitals to provide centralized services, deploy ambulance fleets, and establish cold-chain logistics for medical supplies. This model has worked in developed nations with decades for gradual implementation and substantial capital reserves. Rapidly urbanizing cities in the Global South, however, lack these fundamental prerequisites. For example, Dhaka’s metropolitan population of 25 million grows 3% annually, adding 750,000 people yearly, with one-third living in informal settlements lacking water and sanitation; seasonal flooding contaminates supplies, spreading waterborne diseases across densely packed neighborhoods (MacroTrends, 2024a; UNDP, 2019). Karachi faces even more severe constraints: 20.3 million people experience near-daily 8-12 hour power outages, while 62% live in informal settlements without clean water access (Hasan, 2020; Pakistan Census, 2023; Pakistan Today, 2024). These cities lack not only the resources to build conventional healthcare infrastructure at scale but also the stable foundational systems (reliable electricity, paved road networks, and supply chains) that traditional hospital-centric models require.
This research examines an alternative paradigm: tech-enabled distributed healthcare systems that use community health workers, digital infrastructure, drone logistics, telemedicine, and AI-driven coordination to deliver healthcare services without requiring extensive traditional physical infrastructure. Rather than assuming eventual development of conventional infrastructure, distributed models operate within existing constraints, deploying healthcare delivery mechanisms adapted to contexts of permanent infrastructure limitation. Implementation evidence from Rwanda and Ghana demonstrates operational feasibility, with documented improvements in delivery times and reductions in medical supply wastage, suggesting that distributed systems can achieve measurable health outcomes in resource-constrained environments.
Drawing on this implementation data, constraint analysis of five representative megacities (Dhaka, Karachi, Lagos, Kinshasa, and Mumbai), and detailed economic modeling for Karachi, this study evaluates whether distributed healthcare represents more than a temporary solution for underserved populations. The central question is whether tech-enabled distributed systems offer the primary viable pathway to health system resilience for rapidly urbanizing cities facing permanent infrastructure constraints.
Beyond questions of efficiency and cost, healthcare access is fundamentally a question of justice. Residents of informal settlements in Dhaka, Karachi, Lagos, and Kinshasa often experience systematic exclusion from healthcare not because of medical need, but because of geographic, economic, and infrastructural barriers. Examining distributed healthcare, therefore, requires consideration not only of service delivery outcomes but also of whether health systems can distribute access to care more equitably among populations historically marginalized by patterns of urban development.
Literature Review
Healthcare infrastructure development in rapidly urbanizing cities of the Global South sits at the center of debates about how to address resource constraints, improve healthcare access, and navigate development pathways and technological adoption. Recent research confirms the limitations of traditional hospital-centric approaches while exploring alternatives better suited to constrained urban contexts.
Hospital-centric models have dominated healthcare planning based on centralized expertise and resource consolidation. Recent research confirms advantages for complex procedures but reveals systematic access problems in rapidly growing cities. Studies show hospital clustering creates uneven distribution and supply-side inequalities in Chinese megacities (Liu et al., 2025) and South Asian cities, where national insurance programs like India’s Ayushman Bharat cover only hospital inpatient care (Swaminathan et al., 2024). Iranian studies show that hospital development is concentrated centrally, while urbanization expands geographically (Rezaee et al., 2021). This centralization paradox shapes infrastructure debates across developing regions.
Distributed healthcare offers an alternative optimized for resource-constrained contexts. Unlike hospital-centric approaches requiring extensive infrastructure, distributed models deploy community health workers, telemedicine, and technology-enabled logistics within existing constraints. Research on maternal and child health argues that cultural contexts of interdependence in less-developed countries advantage collaborative models (Nyamtema et al., 2018). India’s telemedicine experiments show remote consultation works best as one component of well-functioning systems (Sharma & Yadav, 2020). Pakistan’s Novel Hybrid System of Telemedicine demonstrates adaptation for low-resource settings through community platforms (Wali & Khattak, 2018).
Real-world implementations demonstrate operational feasibility. Rwanda’s Zipline network delivers approximately 75% of the nation’s blood supply outside the capital (Kayitana, 2026), while Ghana completes 600+ daily deliveries nationwide. Zipline has expanded to Nigeria, Côte d’Ivoire, Kenya, and other African countries (Zipline, 2026). Research confirms drones maintain proper storage temperatures, addressing supply chain constraints where infrastructure remains unreliable (Nisingizwe et al., 2022). Community health worker programs show comparable results, with India’s eSanjeevani platform improving workload and health outcomes (Shah et al., 2022). AI applications demonstrate potential for optimizing scarce resources through improved scheduling and triage (Alowais et al., 2024).
These implementations intersect with broader theoretical debates on infrastructure development in the Global South. Leapfrogging theory suggests developing countries can bypass traditional stages, moving directly to advanced technologies at lower costs (Custer et al., 2026). Mobile telecommunications exemplifies this, where countries adopted cellular networks without landline infrastructure (Melbourne Microfinance Initiative, 2023). Digital platforms further enable leapfrogging by providing institutional infrastructure, not merely information exchange (Heeks, 2021). However, critics question whether technological adoption addresses underlying governance constraints. Urban planning research increasingly challenges the transitional view of peri-urbanization, instead recognizing permanent constraints and designing solutions optimized for contexts that may never achieve conventional development benchmarks (Follmann, 2022). This tension shapes how researchers conceptualize infrastructure pathways for rapidly urbanizing cities.
From a global justice perspective, healthcare infrastructure is not merely a technical challenge but a question of equitable distribution. Rapid urbanization frequently produces spatial inequalities in which residents of informal settlements face disproportionate barriers to accessing healthcare services. Technologies that reduce these barriers may therefore be evaluated not only by efficiency metrics but also by their capacity to advance more equitable health outcomes.
Methodology
This research uses a mixed-methods approach combining case study analysis, constraint framework development, and economic modeling.
Rwanda and Ghana were selected as primary implementation cases based on operational maturity (Rwanda since 2016, Ghana since 2019), availability of performance data, government commitment to systematic deployment, and documented health outcomes. Data sources include academic studies (The Lancet), government health statistics (Rwanda Ministry of Health, Ghana Health Service), technology provider data (Zipline, Babyl), and national health information systems.
Performance metrics analyzed include delivery times, maternal mortality rates, blood wastage, system costs, and population coverage rates. Baseline comparisons use historical data from the same facilities before distributed system implementation to establish counterfactual scenarios.
Building on these case studies, a constraint-matching framework emerged through iterative analysis of infrastructure conditions, implementation requirements, and system performance across diverse urban contexts. Five primary constraint dimensions were identified through comparison of successful implementations (Rwanda, Ghana) against infrastructure requirements for traditional hospital-centric systems.
-
Population growth rate (annual percentage determining infrastructure gap expansion)
-
Infrastructure deficit (unfunded gaps in facilities, utilities, transport as a percentage of GDP)
-
Geographic and infrastructure barriers (flooding, congestion, poor roads, terrain disrupting delivery)
-
Mobile access (household internet penetration enabling digital interventions)
-
Power disruption (annual outage days affecting cold-chain logistics).
Threshold values for each constraint were established by analyzing conditions in Rwanda and Ghana at the time of successful distributed system deployment, cross-referenced with technical specifications for traditional hospital operations. Cities meeting all five threshold criteria were thought to be optimal contexts for distributed model deployment.
To test this framework, five cities were selected for comparative analysis. Four rapidly urbanizing cities (Dhaka, Karachi, Lagos, and Kinshasa) were chosen based on population exceeding 10 million, annual growth rates above 2%, documented infrastructure deficits, and geographic or climatic challenges. Mumbai was included to test framework boundaries, representing a megacity in the Global South that nevertheless may not meet all constraint criteria.
Data sources include MacroTrends (2024) for population growth, World Bank and national planning documents for infrastructure deficits, World Bank Infrastructure Reports and Numbeo (2022) for geographic barriers, national statistics agencies for mobile access, and utilities data for power disruptions.
The final methodological component involves economic analysis comparing two scenarios for Karachi over a 10-year planning horizon (2026-2035).
Methodological Note: This analysis compares two healthcare delivery models as if each were built from scratch, rather than as additions to Karachi’s existing healthcare system. This “from scratch” comparison allows for a clean evaluation of each model’s cost-effectiveness by avoiding: (1) uncertainty about the capacity and quality of existing facilities; (2) the risk of counting the same population twice when new services overlap with existing ones; (3) difficulty comparing quality between old and new facilities; (4) unclear divisions of costs between existing and new infrastructure. In practice, either model would work alongside Karachi’s current healthcare system.
Regional benchmarks suggest healthcare capacity targets for South Asian megacities: Indonesia maintains approximately 1.0 beds per 1,000 population, Philippines 1.0, and Thailand 2.1. A conservative target of 1.5 beds per 1,000 population is a reasonable goal for a South Asian megacity. By 2035, Karachi’s population will reach 25.3 million, requiring 37,950 total hospital beds at this benchmark.
The models differ fundamentally in their approach to healthcare delivery. The traditional model addresses all healthcare needs through hospital-based services. The distributed model recognizes that primary healthcare addresses more than 80% of people’s common health needs (PHCPI, 2022), allocating this proportion to community health workers who provide care directly in communities, with hospitals sized for the 20% of needs requiring specialized care, emergency services, and surgical interventions.
The traditional model assumes 190 hospitals (200 beds each) built over 8 years to achieve 1.5 beds per 1,000 population, with approximately 24 hospitals initiated annually given Pakistan’s 2-year build cycle. Hospital construction costs approximately $70 million per facility (Appendix A.1), with operating costs of $12,099 per bed annually (Appendix A.2). Costs distribute evenly across the 2-year construction period, with operating costs beginning when facilities open.
The 190 hospitals provide 38,000 beds (1.5 per 1,000 population), but three barriers limit access. Spatial barriers prevent access from approximately 62% of residents in ‘katchi abadis’ with narrow lanes impassable to ambulances (Hasan, 2020). Economic barriers arise from substantial out-of-pocket costs. Structural barriers emerge from poor integration between settlement clinics and hospitals, creating fragmented care pathways.
The distributed model deploys 38 hospitals (7,600 beds), 12,000 community health workers, drone networks, telemedicine platforms, and AI logistics. Capital costs total $2.70 billion: hospitals ($2.66B, Appendix A.1), CHW training ($5.2M, Appendix A.3), drones ($15.6M, Appendix A.4), digital platforms ($8M, Appendix A.5), and AI systems ($12M, Appendix A.6). Operating costs total $113.7 million annually: hospitals ($91.9M, Appendix A.2), CHWs ($13.37M, Appendix A.3), drones ($3.9M, Appendix A.4), digital platforms ($1.5M, Appendix A.5), and AI ($3M, Appendix A.6).
Cost estimates are projections from comparable implementations in Rwanda, Ghana, Pakistan, and India, adjusted for Karachi’s scale. Actual costs may vary based on procurement, wages, and technology selection. Estimates use conservative assumptions favoring higher costs.
Deployment follows a phased 8-year timeline with capacity ramping from 10% (Year 1) to 100% (Year 8). Hospital construction requires 2 years, with 10 hospitals starting each year in Years 1-4. CHW programs expand over 8 years, drones deploy over 3 years, digital infrastructure in 2 years, and AI in Years 2-3. Operating costs scale with capacity.
The distributed model provides 7,600 beds (0.30 per 1,000 population), below the 1.5 benchmark because 80% of health needs are addressed by community health workers, while hospitals handle specialized care, emergencies, and surgery.
Results
Real-world implementations in Rwanda and Ghana demonstrate the operational viability and health impact of distributed healthcare systems. Rwanda’s national drone delivery network, operational since 2016, serves health facilities across the country’s territory. The system delivers blood products, vaccines, and emergency medical supplies to facilities previously requiring 4+ hours by road transport. Compared to traditional ground transport averaging 139 minutes (2.3 hours), drone delivery reduced average delivery time to 41 minutes, which is 70% faster. Blood product waste decreased substantially, with a 67% reduction in expirations at 12 months after implementation (Nisingizwe et al., 2022).
Ghana’s implementation since 2019 serves over 2,000 health facilities across four hubs, completing 600+ deliveries daily. Rwanda’s e-Ubuzima platform integrates electronic health records nationally. Babyl Rwanda processed 3.9 million telemedicine consultations between 2019-2023 (Rubuga et al., 2026), while community health insurance (Mutuelle de Santé) covers 90% of the population. An AI training platform supports 58,567 community health workers (CIICHIN, 2025; Rwanda Biomedical Centre, 2025).
Application of the constraint framework to five megacities identifies distinct patterns (Table 1). Dhaka, Karachi, Lagos, and Kinshasa meet all five criteria, while Mumbai met only three, with more developed infrastructure making traditional models viable.
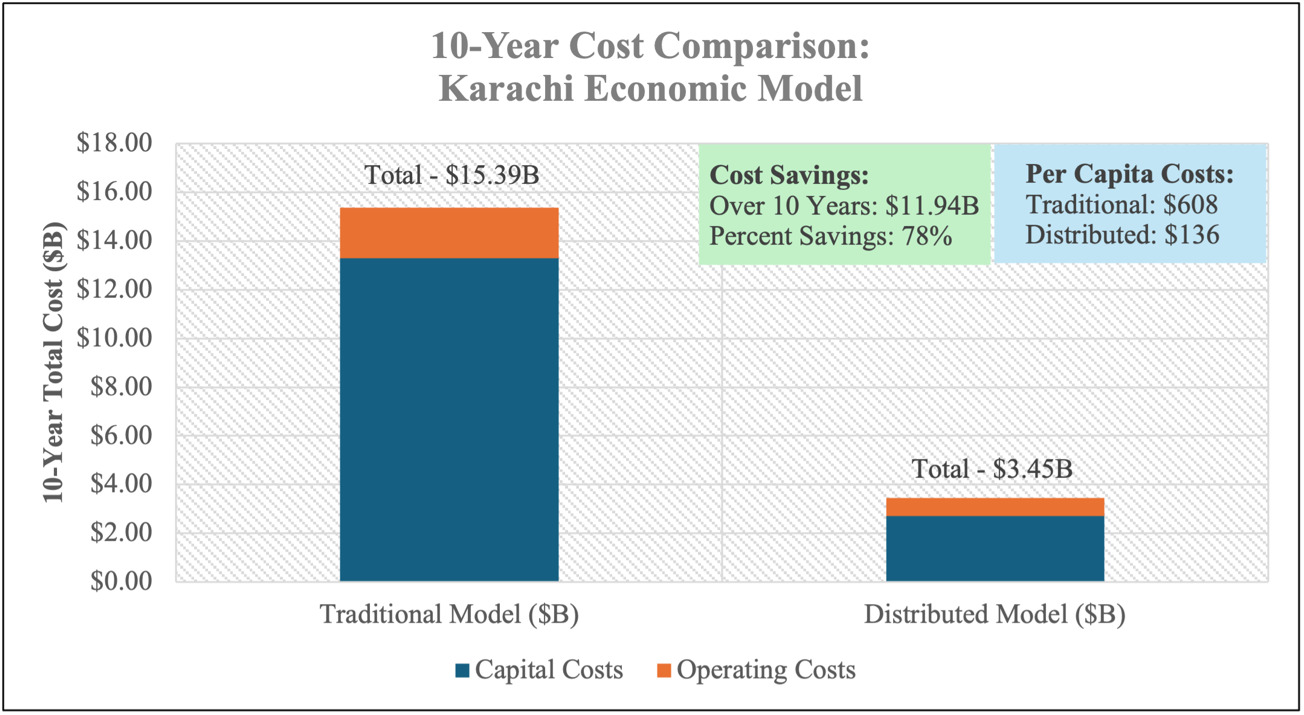
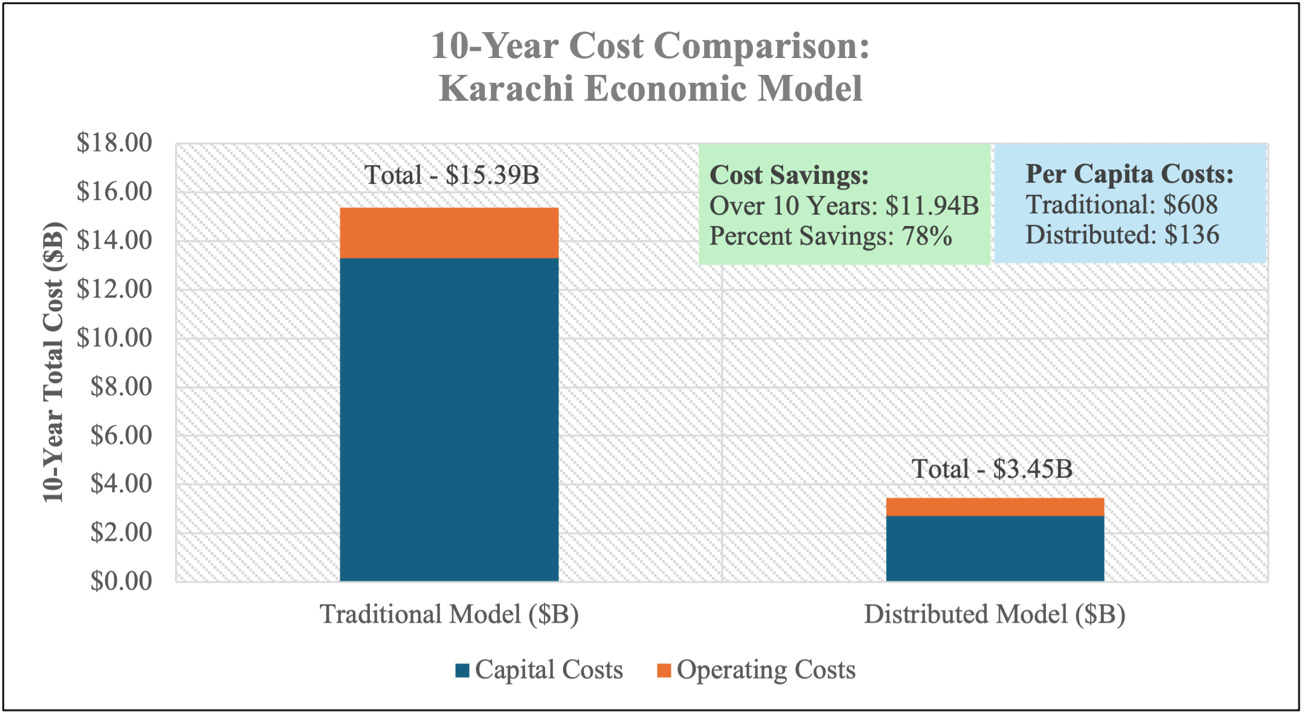
The economic analysis of Karachi demonstrates substantial cost and coverage advantages for the distributed model.
The traditional model requires $15.39 billion total investment over 10 years, achieving 55% population coverage (13.9 million people) due to spatial and economic barriers limiting access. The distributed model achieves 100% population coverage (25.3 million people) at $3.45 billion total investment, delivering $11.94 billion in cost savings (78% reduction). Per capita costs total $136 for the distributed model versus $608 for traditional infrastructure. Figure 1 illustrates the year-by-year cost comparison.
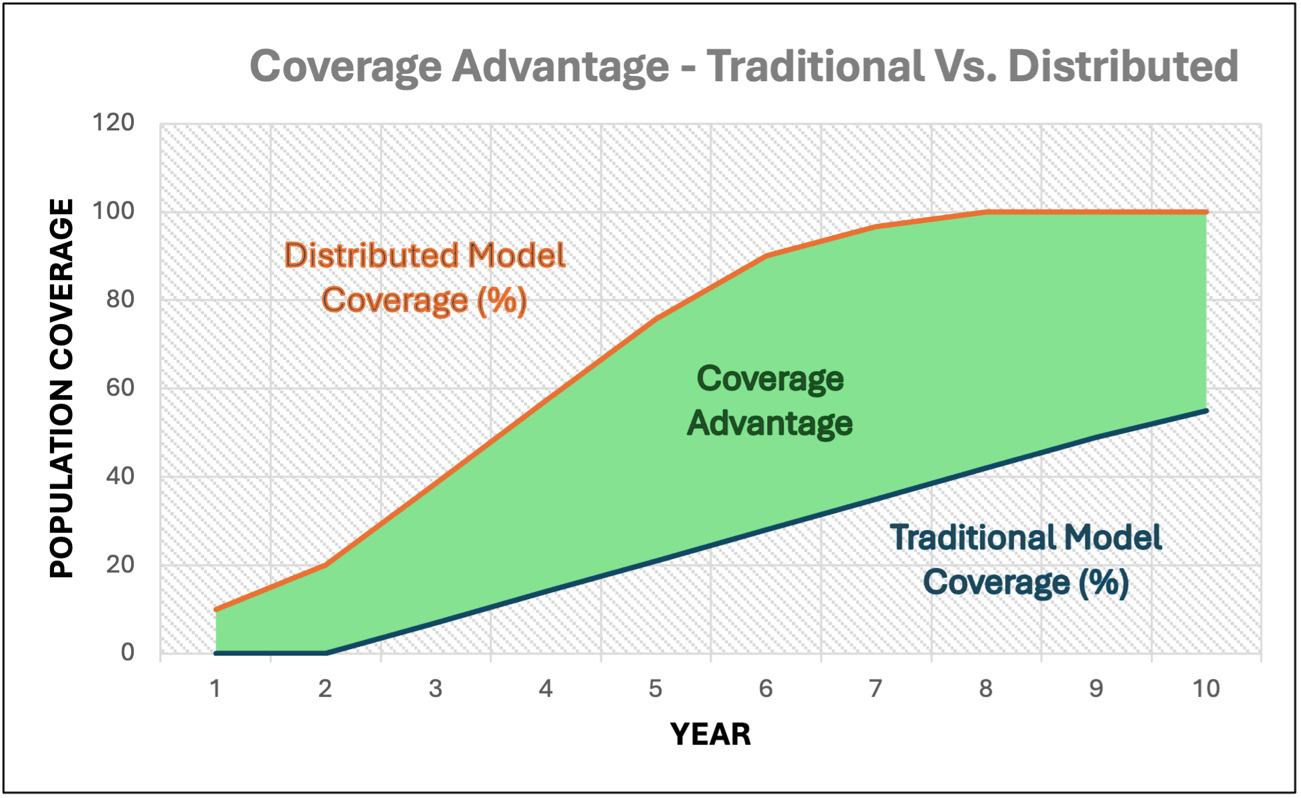
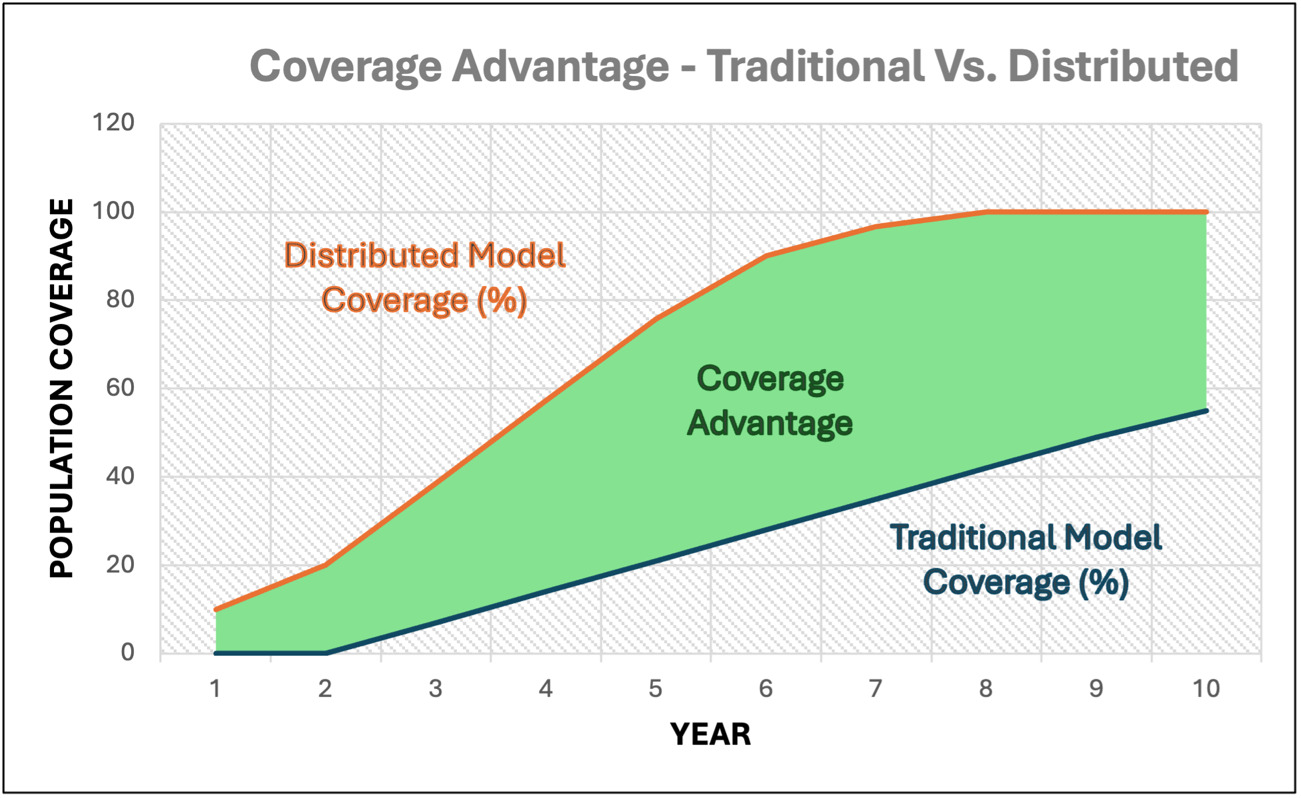
Coverage progression demonstrates significant time advantages (Figure 2). The distributed model reaches 100% population coverage by Year 8, while the traditional model reaches only 55% by Year 10. The distributed model achieves 50% coverage in Year 4, five years faster than the traditional model’s Year 9 milestone. Coverage is calculated using weighted system readiness methodology: Coverage = (CHW deployment readiness × 0.8) + (hospital deployment readiness × 0.2), where weights reflect that primary care addresses 80% and specialized care addresses 20% of population health needs (PHCPI, 2022). This accounts for the distributed model’s 38 hospitals with 7,600 beds serving specialized care, complemented by 12,000 community health workers providing primary care, compared to the traditional model’s 190 hospitals with 38,000 beds addressing all healthcare needs through hospital-based services.
Discussion
This research challenges basic assumptions about healthcare infrastructure development in resource-constrained urban environments. The results show that distributed models are not just cheaper versions of traditional healthcare. They represent fundamentally different solutions designed specifically for cities that will never have full infrastructure.
The distributed model works precisely because it operates within these constraints rather than assuming their resolution. Drone networks function during power outages and flood conditions. Telemedicine platforms use existing mobile infrastructure rather than requiring new transportation networks. Community health workers reach areas where traditional facilities face access challenges. AI logistics optimize scarce resources rather than assuming abundance. The model achieves 100% population coverage by Year 8 when both CHW and hospital components reach full deployment, establishing healthcare delivery mechanisms adapted to the city’s actual conditions rather than requiring the city to develop infrastructure conditions that may never materialize.
Economic modeling shows time advantages as important as cost savings. The distributed model reaches 50% coverage in Year 4 versus Year 9 for traditional infrastructure, a five-year acceleration where 500,000-600,000 new residents arrive annually. Each year of delay means hundreds of thousands without healthcare access. This time dimension receives insufficient attention in development literature.
These findings have direct implications for policy frameworks. Implementation requires policy frameworks distinct from traditional approaches. Regulatory environments must accommodate urban drone operations and telemedicine licensing. Current regulations in most developing nations assume ground-based delivery and in-person consultations, creating legal barriers.
Government procurement systems require adaptation. Traditional infrastructure procurement focuses on construction contracts for discrete facilities. Distributed systems require integrated technology platforms, continuous software updates, and ongoing training programs. Financing mechanisms must shift from capital-intensive hospital construction to operating-expense-intensive technology deployment.
The 45 percentage point coverage advantage (100% versus 55%) has implications for urban health policy. Traditional infrastructure concentrates benefits in areas with road access and formal addresses. Distributed systems extend coverage more broadly across the city’s geography, creating different implementation priorities for health system governance. International development institutions must reconsider funding priorities. Current development assistance emphasizes hospital construction and physician training while providing limited support for technology infrastructure, community health worker programs, or AI system deployment.
The findings also carry broader implications for global justice. Healthcare exclusion in rapidly urbanizing cities is often concentrated among populations living in informal settlements, migrant communities, and low-income households. Traditional hospital-centered systems frequently privilege populations located near formal infrastructure while leaving marginalized communities underserved. Distributed healthcare models may help reduce these inequities by bringing services directly into communities that have historically been excluded from healthcare systems. In this sense, the significance of distributed healthcare extends beyond efficiency or cost reduction; it concerns the ability of health systems to recognize the equal moral worth of populations whose healthcare needs have often been overlooked in conventional development planning.
Along with substantial policy implications, several significant counterarguments warrant careful consideration. While this research demonstrates distributed healthcare’s advantages in constrained contexts, critics raise legitimate concerns about governance capacity, ethical implications of AI-driven coordination, and technological dependency that merit substantive engagement.
Governance instability represents a fundamental challenge in rapidly urbanizing cities with weak institutional capacity. Critics argue complex technology systems cannot function in such environments. However, distributed systems may prove more resilient than traditional infrastructure. Hospital-centric models require sustained governance for construction oversight and facility management. Distributed models distribute operational control across workers and technology platforms, reducing vulnerability to failures at any single point.
Ethical concerns about AI-driven coordination merit serious attention. Algorithmic bias, privacy vulnerabilities, and accountability gaps pose real risks. The model’s reliance on AI for resource allocation requires proactive mitigation through transparent algorithms, regular bias audits, clear accountability frameworks, and ongoing ethical review. The open-source nature of platforms like DHIS2 enables local scrutiny, while AI systems must embed ethical protections from inception.
Dependence on foreign technology providers creates legitimate sustainability concerns. However, this critique applies equally to traditional infrastructure dependent on imported medical equipment and pharmaceuticals. The distinction lies in technology transfer potential. Software platforms enable knowledge transfer through open-source code and local developer training. Rwanda and Ghana demonstrate progression from implementation to local adaptation.
Beyond these counterarguments, this research faces several limitations that constrain generalizability. The economic modeling relies on cost estimates from vendor quotes, government procurement records, and academic studies rather than actual implementation data in Karachi specifically. The constraint framework uses threshold values established through analysis of Rwanda and Ghana implementations, which differ substantially from megacities like Dhaka, Karachi, Lagos, and Kinshasa in population scale, density, and institutional capacity.
The analysis assumes technology performance equivalent to Rwanda and Ghana. However, megacities present greater airspace congestion, higher demand loads, and larger patient populations. These scaling challenges may reduce performance or increase costs beyond projections.
Physician shortages pose a constraint not fully addressed by distributed systems. While CHWs and telemedicine extend reach, complex procedures require physicians. Rwanda maintains 1.2 physicians per 10,000 population versus WHO’s recommended 10 per 10,000. Distributed systems improve access but cannot resolve workforce shortages without parallel medical education investments.
In addition, weather vulnerabilities affect drone operations. Heavy rain, high winds, and extreme heat ground drone fleets. Funding sustainability remains uncertain as implementations benefit from international development assistance and philanthropic support that may not continue indefinitely.
The framework’s generalizability extends to other rapidly urbanizing cities beyond the five analyzed, including Luanda, Dar es Salaam, Nairobi, Kolkata, Hyderabad, Lahore, Jakarta, and Manila. Each context requires adapted implementation reflecting local conditions. Future research should prioritize pilot implementations, longitudinal health outcome studies, comparative analyses, technology transfer pathways, and political economy investigations of equity impacts.
Conclusion
This research shows that tech-enabled distributed healthcare offers the primary viable solution for rapidly urbanizing cities facing permanent infrastructure constraints. Evidence from Rwanda and Ghana confirms operational feasibility and measurable health impact. The constraint-matching framework identifies conditions where distributed models outperform traditional approaches. Economic modeling finds substantial cost savings, coverage advantages, and time benefits.
For cities meeting the framework criteria, distributed healthcare is not an incremental improvement but a qualitatively different solution optimized for constrained contexts. The Karachi analysis shows the distributed model’s dramatic advantages in cost efficiency, population coverage, and deployment speed. The model deploys healthcare delivery mechanisms that function within the city’s actual infrastructure conditions, including areas where spatial and economic barriers limit traditional hospital access.
Key limitations include physician shortages, weather vulnerabilities, technology dependence, and funding sustainability. But these constraints affect traditional models equally or more severely. Cities lacking resources for hospital construction, road networks, and reliable electricity cannot overcome these limitations through conventional approaches within actionable timeframes. The choice for these cities is not between distributed systems and ideal hospital-centric infrastructure but between distributed systems and continued inadequate healthcare access across their growing populations.
The implications extend beyond healthcare to broader questions about infrastructure development in resource-constrained contexts. When traditional development pathways require resources and timeframes unavailable to rapidly growing cities, alternative models optimized for permanent constraints become necessary rather than optional. Ultimately, the challenge facing rapidly urbanizing cities is not simply how to build healthcare systems more efficiently, but how to ensure that vulnerable populations are not excluded from lifesaving care because of where they live or the surrounding infrastructure deficits.
Distributed healthcare offers a pathway toward greater health equity by extending access to populations that conventional systems frequently fail to reach. As such, its significance lies not only in technological innovation but also in its potential contribution to a more just distribution of healthcare opportunities in the world’s fastest-growing cities. For the billions of people who will live in these cities over the coming decades, distributed healthcare offers not merely a solution but the only realistic path to health system resilience.
Conflicts of Interest
The author declares no conflicts of interest related to this research.
Appendix A: Detailed Cost Estimation Methodology
A.1 Hospital Construction Costs
Hospital construction cost estimates are derived from four recent Pakistani tertiary hospital projects adjusted for inflation to 2026 values:
-
Shaukat Khanum Memorial Cancer Hospital Karachi: Rs 30 billion for 400 beds (2023) - Source: The Nation (2023)
-
PIMS Cancer Hospital Islamabad: Rs 10.8 billion for 200 beds (2023) - Source: Dawn (2023b)
-
Peshawar IFC Tertiary Care Hospital: Rs 20 billion for 500 beds (2022) - Source: Dawn (2022)
-
National Police Hospital Islamabad: Rs 6.48 billion for 100 beds (2023) - Source: Dawn (2023a)
Pakistan cumulative inflation rates (WorldData, 2025): 75% (2022-2026), 61.2% (2023-2026). Each project’s per-bed cost was inflation-adjusted to 2026 values, scaled to 200-bed facilities, and averaged.
Final estimate: $70 million per 200-bed tertiary hospital (2026 values)
A.2. Operating Cost Adjustments
Operating costs use Indian district hospital data from Chatterjee et al. (2013): 400-bed hospital at Rs. 394 per bed-day (2010-11). Adjusted for Pakistan’s 8.7% average annual inflation (2011-2026) yields $9,680 per bed annually, increased by 25% for administration and overhead.
Final estimate: $12,099 per bed annually (2026 values)
Indian data provides the most appropriate benchmark due to geographic proximity, comparable healthcare systems, similar patient populations, and peer-reviewed data quality from government facilities.
A.3. Community Health Worker Costs
Based on Pakistan’s Lady Health Worker program (Lok Sujag, 2025):
-
CHW salary: PKR 25,000 monthly (~$1,071 annually)
-
Supervisor salary: PKR 30,000 monthly
-
Supervisory ratio: 1:30
For 12,000 CHWs:
-
Annual salaries: $12.85M (CHWs) + $0.51M (400 supervisors) = $13.37M
-
Capital: $200K (training) + $5M (equipment: mobile devices, medical kits, transportation) = $5.2M
A.4. Drone Delivery Network Costs
Scaled from Ghana’s Zipline implementation (Siebert et al., 2019; Wikipedia, 2025): $12.5M for 4 distribution centers serving 600 daily deliveries. Karachi’s urban density (26,000+ persons/km²) enables higher efficiency than rural deployment. Research shows urban drone delivery achieves significantly higher route efficiency due to shorter distances and higher delivery density (FreightAmigo, 2025).
For Karachi (5 distribution centers):
-
Capital: $15.6M (infrastructure, drone fleet, landing/charging stations, control systems)
-
Annual operating: $3.9M (maintenance, personnel, energy, communications)
A.5. Digital Health Platform Costs
DHIS2 (District Health Information Software 2) is free open-source software used nationally in 75+ countries, with national-scale rollouts typically requiring 6-12 months (DHIS2, 2025).
Capital ($8M total):
-
Infrastructure and hosting: $3M
-
Configuration and customization: $3M
-
Training: $2M
Annual operating: $1.5M (cloud hosting, updates, technical support, system monitoring)
A.6. AI Analytics System Costs
City-scale AI deployment for hospital coordination, CHW routing, drone logistics, demand forecasting, and supply chain optimization (Aalpha, 2026).
Capital ($12M total):
-
Custom model development: $7M
-
Cloud infrastructure: $3M
-
System integration: $2M
Annual operating: $3M (cloud operations, model retraining, maintenance)
Note: All estimates use conservative assumptions favoring higher costs. Actual costs may vary based on procurement negotiations, local wage levels, technology provider selection, and implementation approaches.